Recurrent Sublumbar Abscesses Due to Occult Grass Seed
Clinical Connections – Summer 2025
Grace Thomas (Resident in Small Animal Surgery)

Norman, a three-year-old cocker spaniel, presented to our Emergency Referrals Service last October, following a two-day history of lethargy, inappetence, pyrexia and a vomiting episode.
Investigations performed on admission confirmed a septic peritoneal effusion, suspected to be secondary to right-sided sublumbar abscessation.
Norman was taken to surgery overnight for an exploratory laparotomy. Generalised peritonitis was found and a large, leaking sublumbar abscess was identified, explored and flushed. No perforations of the gastrointestinal tract were found, and no foreign material was identified in the abscess or the surrounding fibrous tissue.
After the sublumbar abscess and abdomen were copiously lavaged, an active suction abdominal drain was placed and the abdomen was closed routinely.
Norman spent five days recovering in the Queen Mother Hospital for Animals (QMHA) and made good progress. As fluid production had subsided, the abdominal drain was removed the day before discharge. A nasogastric tube that had been placed to support nutrition in the postoperative period had been removed the day before as he was eating well.
He was discharged from the QMHA with a four-week prescription of amoxiclav. Norman’s owners were cautioned about the possibility of recurrence of the sublumbar abscess, as an underlying inciting cause had not been identified. They were advised to have Noman re-examined if he developed any signs of recurrence, including lethargy, inappetence, pyrexia, lameness, and lumbar or abdominal pain.
Second admission
Almost a month later Norman was brought back to the QMHA due to signs of lethargy and pyrexia. CT of the thorax and abdomen confirmed the suspected recurrence of a sublumbar abscess, but an inciting cause remained elusive.
Norman was again taken to surgery for an exploratory laparotomy, where a large, sublumbar abscess was identified, opened, explored, debrided and flushed. No foreign material was identified in the abscess or surrounding fibrous tissue. The sublumbar abscess and abdomen were copiously lavaged. As previously, an active suction abdominal drain was placed, and the abdomen was closed routinely.
Norman recovered well and the abdominal drain was removed five days after admission as fluid production had subsided. He was discharged the following day, with a two-week course of amoxiclav, to be followed by four more weeks. As no inciting cause was found, the risk of recurrence was reiterated to owners, and they were advised to have him re-examined if signs of recurrence were observed.
Third admission – underlying cause identified
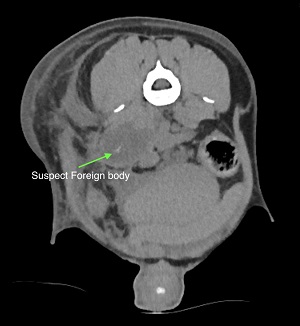
Norman was returned to the RVC two months later, following a recurrence of previous symptoms. Abdominal CT confirmed a recurrence of a sublumbar abscess and a suspect foreign body visible in the caudal aspect of the abscess, ventral to the transverse process of the L7 vertebra.
After deliberation, Norman's owners opted to proceed with further surgery. An exploratory laparotomy identified a large, sublumbar abscess – and a grass seed was retrieved using intraoperative ultrasound guidance.
The abscess had begun to leak into the abdomen, causing generalised peritonitis. The sublumbar abscess was opened and debrided extensively, and the abdomen was copiously lavaged. An active suction abdominal drain was placed and the abdomen closed.
Norman also had fairly extensive abdominal adhesions. Some of them were removed for surgical access to the abscess, but many around the GI tract were left. Further abdominal surgery would likely be challenging due to the adhesions, which would be expected to progress further following the most recent surgery.
Recovery
Norman made excellent progress postoperatively and his abdominal drain was removed two says after surgery. He was discharged the following day with the same antibiotic course as before as well as an NSAID and an analgesic.
The day after discharge Norman presented to the out-of-hours service after interfering with his surgical wound – he had managed to remove his buster collar and lick his wound.
The surgical wound was dry but there were two areas where the skin was slightly open. Following recommendation from the Emergency and Critical Care team, Norman's wound was cleaned and three staples placed on the areas where the skin was open. A body suit was placed before he returned home.
His owner Jack informed us that he is doing “brilliantly” and is back to his normal self: “swimming, racing around and living and loving life to the full.”