Medicine Nursing at the Queen Mother Hospital for Animals
Clinical Connections – Autumn 2016
With nurses playing such a vital role at the Queen Mother Hospital for Animals (QMHA), we thought readers would be interested to discover how our medicine nursing team works. This article by RVN Gina Parkes, who has a DipAVN qualification, offers an overview of the medicine nurse role at the hospital, illustrated with a case example.
Introduction
The QMHA team includes some of the most skilled RVNs in the UK, many of whom have advanced qualifications in their fields. They have expertise in caring for some of the most challenging cases seen in veterinary practice.
The QMHA nursing team consists of 90 nurses, divided into the specialisms of medicine, oncology, emergency and critical care, anaesthesia, neurology, surgery and theatre. As the Head Medicine Nurse, I am fortunate to lead a team of 15 highly skilled nurses who are responsible for the co-ordination and management of the endoscopy and laser suite, radioactive iodine unit and isolation ward.
Advanced nursing care includes enteral feeding tube placement and management, cephalic and arterial blood gas analysis, pain scoring and multimodal pain relief administration. Medicine nurses also assist with procedures like bone marrow biopsies and joint taps.
The hospital works in a transdisciplinary manner, involving a great deal of interaction between the different teams to ensure the best results for each patient.
As the QMHA is a teaching hospital, each working day includes the guidance of veterinary and veterinary nursing students in their final years of training. A large part of our role includes the teaching of students, including in phlebotomy skills, patient handling and supervision during patient care.
Case Study
Laser ablation of bilateral ureteral stenosis
- Male neutered medium crossbreed, 35.2kg
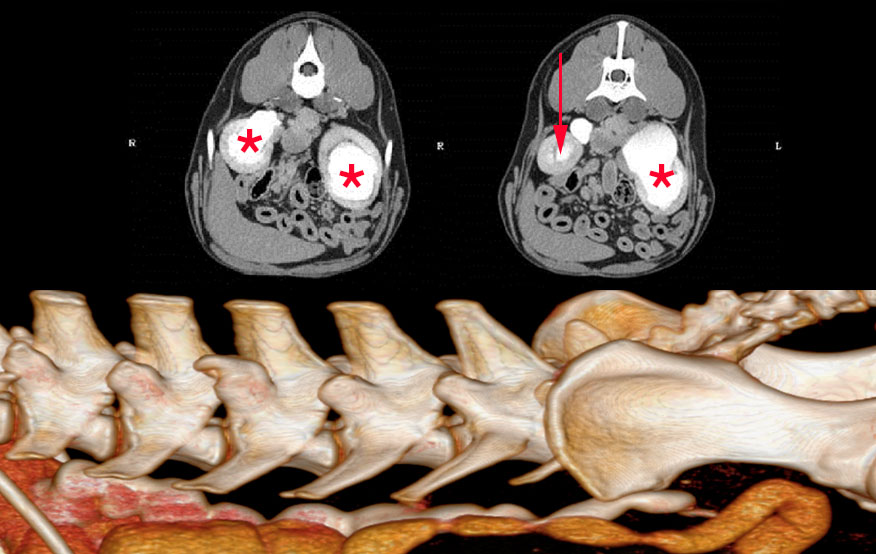
The patient presented to the QMHA with previously diagnosed bilateral mega ureters with hydronephosis, causing urinary tract complications. There were concerns that renal function could deteriorate if untreated. Peripheral catheterisation of the cephalic vein was carried out by a student under the supervision of a medicine nurse. Blood samples were also taken from the jugular vein for biochemistry panel analysis, including renal values. CT excretory urogram under sedation revealed severe dilation of the left and right renal pelves and ureters, with a radiological conclusion of severe hydronephrosis and hydroureter. There was no evidence of mechanical ureteric obstruction but reduced emptying of urine from the kidneys to bladder suggested bilateral ureteral stenosis. An appointment for urinary tract endoscopy and laser ablation to increase the size of the ureterovesicular orifice was arranged. The role of the medicine nurse for this procedure included:
- Selection and preparation of required equipment, including adapters/extension sets for use through the scope, hydrophilic guidewires, urinary and ureteral catheters, and laser fibres.
- Preparation of laser equipment, including a Lumenis powersuite holmium laser, non-return valve adapters and a 395 micron slim-line laser fibre.
- Selection of the correct fibre and examination for damage and loss of accuracy, before sterilisation.
- Selection of the scope - a male canine flexible ureterocystoscope, sterilised using ethylene oxide.
- Laser safety attendant – ensuring safety equipment such as goggles and warning signs were used and switching the laser into standby mode when not in use.
- Ensuring the patient and clinicians were prepared and gowned in a sterile manner.
- Preparation of the patient - caudal abdomen and inguinal area was clipped and scrubbed and the prepuce was flushed using saline.
- Provision of equipment throughout procedure and attachment of the saline flush to the scope in a sterile manner - to improve the fluidity of manoeuvres, reduce trauma and improve imaging.
Visualisation of the ureteral openings showed both opened into the correct position within the bladder. Catheterisation of the left ureter was performed and the laser used to enlarge the opening by ablating the stenosed tissue. Post-lasering fluoroscopy revealed improved flow of contrast agent from the ureter into the bladder. Following the procedure, the patient was monitored by the medicine nurses on the ward for 24 hours, where fluids, nutrition and urinary function were monitored. The right ureter was successfully ablated three weeks later.
Sign up to get Clinical Connections in your inbox rvc.ac.uk/clinical-connections