Gait Analysis
Clinical Connections – Summer 2017
Andy Fiske-Jackson, Lecturer in Equine Surgery
Henry, an eight-year-old thoroughbred gelding, was brought in from the field lame four weeks prior to presentation. The referring vet identified a right hind lameness that failed to respond to rest. Subsequent nerve blocks were attempted in the right hind but Henry’s excitable nature precluded further nerve blocks from being placed. He was referred to RVC Equine Hospital for investigation.
On examination
At the hospital, inertial measurement units (IMUs), an objective gait analysis system, were applied to Henry’s lameness and to evaluate any change in the lameness following nerve blocks.
In the past, objective gait analysis required a dedicated gait laboratory with force plates embedded in the floor or retro-reflective markers placed on the horse with their position recorded using three-dimensional computerised motion analysis cameras. Such hi-tech equipment is used in the RVC’s Structure and Motion Laboratory but this approach is not practical even in a referral hospital setting as data collection is too time-consuming. The advent of IMUs allows objective gait analysis to be performed in the field, or hospital setting, in a time efficient manner.
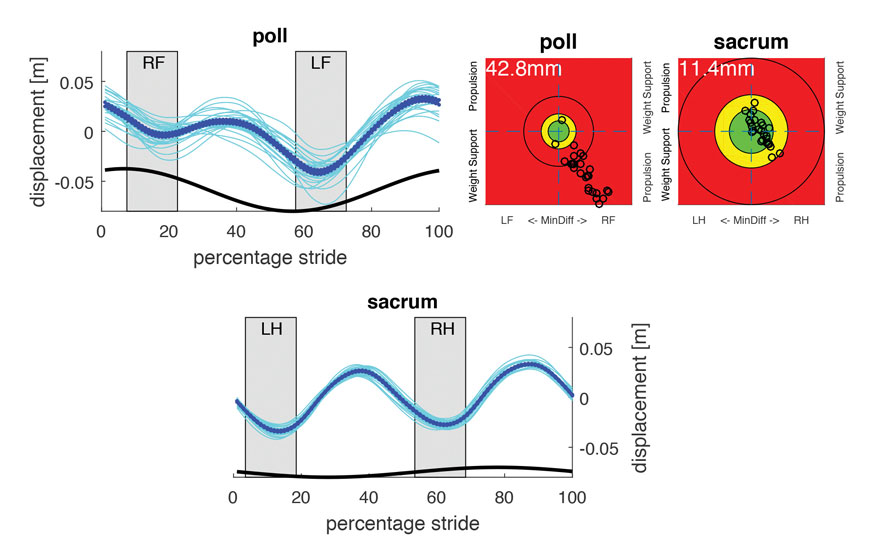
Henry’s initial assessment gave us an unexpected result. There was no significant hindlimb lameness present but a clear right forelimb lameness was identified (Figure 1).
Palpation found no significant localising abnormalities and a lameness work-up using diagnostic anaesthesia (nerve blocks) was begun. Despite 90% of forelimb lameness emanating from the foot, this was not the case with Henry. Nerve blocks were sequentially placed up the limb until a significant improvement was identified with the sensors when the origin of the suspensory ligament was blocked. A similar improvement was also seen 40 minutes after the middle carpal joint was blocked. Ultrasound assessment found a lesion in the suspensory ligament, which was subsequently medicated with platelet rich plasma.

After four months, Henry was sound and work was introduced. Three months later, lameness recurred. The objective gait analysis system was used again and on this occasion no improvement was seen when the suspensory ligament was blocked but improvement was seen 40 minutes after the middle carpal joint was blocked, as in the previous lameness work-up. A standing MRI scan identified subtle osteoarthritis of the right carpus and the joint was subsequently medicated with corticosteroid. Henry was sound during a follow-up appointment and now, five months later, Henry is in full work and remains sound.
Gait analysis system
RVC objective gait analysis system has substantial benefits. Orthopaedic examination and subsequent diagnostic work-up is a complex decision-making process reliant on observation of the horse under a variety of conditions. Mentally retaining such an array of information, some of which may not be consistent, is challenging and prone to expectation bias i.e. a pre-conceived idea of the cause of the horse’s lameness. Therefore, an objective lameness detection system, which can also quantify the degree of lameness, is invaluable. The response to nerve blocks is also very useful, and having the gait analysis system to confirm an improvement, or not, is reassuring.
The large amount of data generated by IMUs, and the ability to detect which part of the stride cycle is affected, may ultimately allow us to relate some of these additional parameters to specific lameness conditions. This would then enable targeted nerve blocking of those conditions, reducing the time taken to resolve the lameness and the needle sticks required in fractious horses.
For equine referrals - please contact RVC Equine on 01707 666667 or equinehospital@rvc.ac.uk