Canine Hypophysectomy Progress
Clinical Connections – Autumn 2018
By Joe Fenn, Lecturer in Veterinary Neurology and Neurosurgery, and Rebecca Geddes, Lecturer in Small Animal Internal Medicine
Following on from the success of feline hypophysectomy procedures performed at the RVC to treat acromegaly and diabetes mellitus in cats, specialists at RVC Small Animal Referrals are using this procedure to treat dogs with pituitary-dependent hyperadrenocorticism (PDH, Cushing’s disease).
Although the underlying cause of PDH in dogs is typically an adrenocorticotropic hormone (ACTH) producing tumour of the pituitary gland, treatment options for PDH have traditionally focused on the management of the resulting corticosteroid excess, using medications such as trilostane.
Therapy for PDH targeting the pituitary tumour itself involves either radiation therapy or surgical excision of the pituitary gland and associated tumour (hypophysectomy). Although radiation therapy has been shown to reduce the size of pituitary masses in dogs, it has a limited effect in terms of reducing the endocrine signs that are the hallmark of PDH.
More recently, a small number of centres in Europe and the USA have been able to offer hypophysectomy as a treatment for PDH in dogs, with very encouraging results. Studies including large numbers of dogs have shown consistent responses to treatment and high rates of sustained remission of endocrine signs in dogs with PDH treated by hypophysectomy. We are excited to offer this excellent treatment option for dogs otherwise faced with a potentially serious and debilitating lifelong condition.
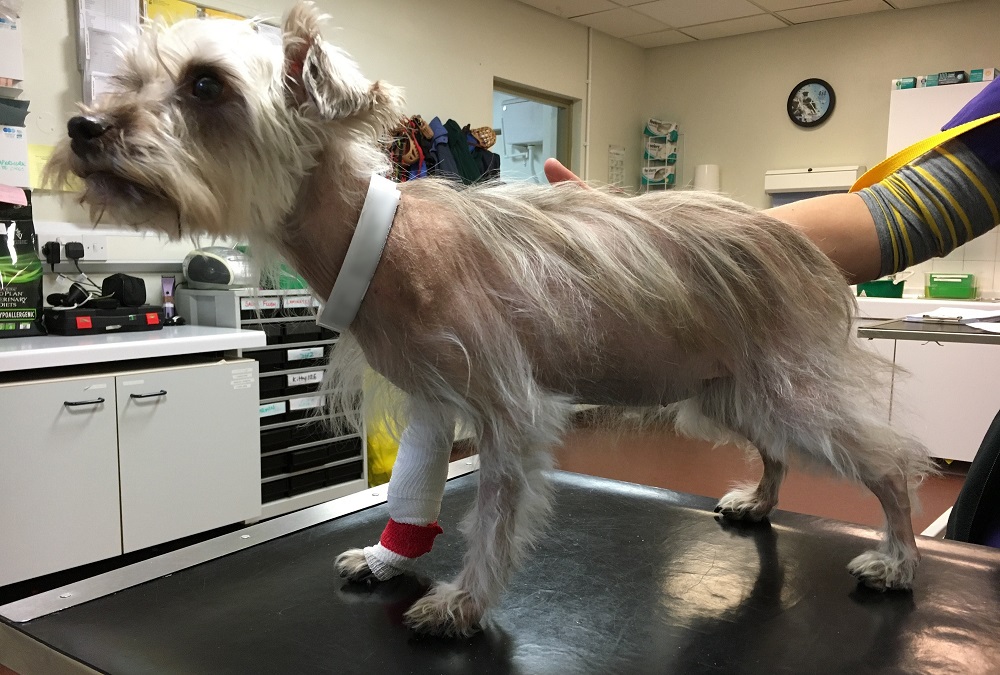
A recent example of the benefits in such a case was Poppy, a six-year-old female neutered miniature schnauzer with a history of PDH that was poorly responsive to medical management with trilostane. She presented to our Internal Medicine Service with an 11-month history of polyuria-polydipsia, polyphagia, loss of muscle condition and progressive alopecia, despite eight months of treatment with escalating doses of trilostane. At presentation to the RVC she was receiving 20mg/kg trilostane once daily, but despite this had recently developed calcinosis cutis (see Figure 1).
As a result, Poppy’s owners elected for her to undergo surgical management of her PDH and she was booked in for a hypophysectomy procedure to remove her overactive pituitary gland. Surgeons from our Neurology and Neurosurgery Service performed the surgery by positioning Poppy in a neurosurgical head-frame and operating through her soft palate to remove the pituitary gland, with no major complications. Poppy recovered rapidly following the anaesthetic and was walking, eating and drinking within hours of the procedure.
As the procedure involved removing the entire pituitary gland, she was managed post-operatively with hydrocortisone, levothyroxine and desmopressin eye drops. Poppy has subsequently been weaned off the eye drops, which is possible in most cases, but she will continue to receive the two other medications long-term.
Poppy demonstrated an excellent recovery and following discharge only three days after the procedure, her clinical signs associated with the PDH began to gradually resolve. By five weeks post-operatively her coat and body condition had already markedly improved (with resolution of her calcinosis cutis) and at her three-month re-examination she appeared clinically normal (see Figure 2). Poppy’s owners report that her quality of life is excellent and that she behaves like a lively puppy again. She continues to do well with no sign of recurrence of PDH almost a year following surgery.

One of the keys to Poppy’s successful outcome was the early diagnosis and referral that allowed our surgeons to operate while her pituitary gland was still relatively small. Research in dogs undergoing hypophysectomy for treatment of PDH has shown that better outcomes are associated with a smaller pituitary mass, emphasising the importance of early diagnosis and advanced imaging in dogs with PDH.
At RVC Small Animal Referrals we are keen to discuss surgical options for the treatment of all cases of hyperadrenocorticism, as in many cases these can offer improved management of clinical signs and are a competitive cost option in the long term.
If you would like to refer or to discuss a potential case with the RVC Internal Medicine or Neurology and Neurosurgery services, please contact us via qmhreception@rvc.ac.uk or on 01707 666399.