| Fundamentals of Epidemiology Home | Glossary |
Chapter 1 Workbook: Introduction to Veterinary Epidemiology
Contents
- Aims and Objectives
- What Is Veterinary Epidemiology? (Part 1)
- Snow on Cholera
- Exposures and Outcomes
- Observational and Interventional Epidemiology
- What Is the Role of Epidemiology?
- Types of Epidemiological Investigation
- Using Epidemiology to Investigate a Specific Disease Problem
- The Population Perspective
- (exercise)
- Summary
Aims and Objectives
Aim
To introduce veterinary epidemiology and its role in informing animal
and human health
Objectives
After completing this session, you should be able to:
|
Explain what veterinary epidemiology is |
|
|
Identify an exposure and an outcome in any given study |
|
|
Explain the difference between descriptive and analytic studies, and between observational and interventional epidemiology |
|
|
Express delight and enthusiasm for this study unit and veterinary epidemiology in general, and rush off to start the course immediately |
This chapter should take you about 1 to 2 hours to complete
What is Veterinary Epidemiology? (Part 1)
Several epidemiological problems have been recently reported extensively in the media.
|
Should foot-and-mouth-disease outbreaks be controlled using vaccination? |
|
|
Can sheep become infected with BSE? |
|
|
Do broiler chickens suffer from pain caused by leg weakness? |
|
|
Does use of antibiotics in animals cause antimicrobial resistance in humans? |
Veterinary epidemiology is an integral component of animal health and veterinary public health.
According to Toma et al's Dictionary of Veterinary Epidemiology, epidemiology is:
"The study of the health status of populations."
So in epidemiology, we are concerned with populations rather than individuals.
Both medical and veterinary epidemiology use the same concepts which is why it was considered appropriate to use some historically relevant medical examples in this course.
Epidemiologists often ask "what is the denominator?" - meaning, what is the population from which the cases arose?
By counting the number of health-related events which occur within a specified time in different populations and taking the denominator into account, we can make estimates of the frequency of these events, which we can compare between different populations.
For example, we can compare the bovine brucellosis infection risk between different countries and at different times.
In Colombia the officially reported bovine brucellosis risk in cattle was 1.6 times 10-4 in 1999. The corresponding figure for Bolivia was 5.5.
Comparison is fundamental to veterinary epidemiology.
By examining the differences between those animals within a particular population which have a disease and those who do not, we can improve our understanding of the determinants of a disease.
Here is an example from medical epidemiology. In Vienna, in the 1840s, the obstetrician Ignaz Semmelweis noticed that many women were dying of puerperal fever. He noticed that there were major differences in the maternal mortality rate from puerperal fever between two clinics within one hospital. He then looked for differences between the two clinics which could account for this.
The clinic with the high mortality rate was used to train medical students, and the clinic with the lower mortality rate was used to train midwives.
Semmelweis observed that, as part of their training, medical students performed genital examinations far more often than midwives. Hand-washing was not routine, and Semmelweis suggested that the students' unwashed hands transmitted infection from woman to woman.
He tested his hypothesis by introducing hand-washing with an antiseptic at the first clinic: the maternal mortality rate subsequently fell to below that in the clinic that trained midwives.
![]() Now
work through the interactive exercise before
reading the rest of the topic
Now
work through the interactive exercise before
reading the rest of the topic
What is Veterinary Epidemiology? (Part 2)
The earliest use of the word "epidemiology" was probably in Spain: in 1598, a book about plague called Epidemiología was already in its second edition.
The first documented appearance of the English form of the word was in 1850 when the London Epidemiological Society was formed.
The word derives from the Greek word epidemos - epi meaning "upon" and demos meaning "people".
The ancient Greek physician Hippocrates (born around 460 BC) used
the word epidemeion to refer to diseases that visit the community,
meaning they occurred from time to time, in contrast to endemeion,
diseases which resided within the community. The expression "endemic
disease" comes from this word.
Hippocrates described the distribution of diseases by season, age, climate
and personal behaviour - which is much the same perspective as modern
epidemiologists have.
"Whoever wishes to pursue properly the science of medicine should proceed thus. First he ought to consider what effect each season of the year can produce … He must consider … how the natives are off for water, whether they use marshy, soft waters, or such as are hard and come from rocky heights, or brackish and harsh. The mode of life also of the inhabitants… whether they are heavy drinkers, taking lunch and inactive, or athletic, industrious, eating much and drinking little."
[Hippocrates: On Airs, Waters and Places]
In 1839, a physician called William Farr was made responsible for medical statistics in the Registrar General's office for England and Wales. He set up a system for the routine collection of data on the number and causes of deaths and other vital statistics.
|
Farr used his data to compare the mortality rates among different populations. For example, he compared mortality rates among people of different occupations. The graph opposite shows his figures comparing the mortality rates between clergymen and publicans (men who ran public bars), subdivided by age-group. This is an example of descriptive epidemiology - describing the frequency of specific events or diseases in a particular population. It is also an early example of the use of routine data sources - data about health-related events which are collected systematically. Routine data sources abut animal health available in many countries today include animal census data, slaughter house data and disease surveillance information on notifiable infectious diseases. |
 |
Farr recognised that these data could be used to help understand diseases. He wrote:
"Different classes of the population experience very different rates of mortality … the principal causes of these differences, besides the sex, age and hereditary organization, must be sought in three sources: ordinary occupations of life, supply of warmth and of food, and differential exposure to poisonous effluvia and to destructive agents" (Farr, 1885)
Snow on Cholera
|
Another important figure in the history of epidemiology was John Snow, an anaesthetist in London in the 19th century who is famous for having administered chloroform to Queen Victoria at the birth of two of her children. However he is better known to epidemiologists for his studies of cholera in London. During the 19th century, cholera periodically swept across Europe. London was rather different then - there was no electricity, there were cows and horses in the streets, and standards of hygiene were poor. In 1848-9 there was a severe cholera epidemic in London, with 15 000 recorded deaths. There was considerable debate about the cause of cholera - at the time, the existence of microbes was hotly contested. William Farr had his own ideas on this. He noticed that some areas of London had far more cholera deaths than others (graph opposite), and he wondered what factors might explain this variation. He found that there were more deaths from cholera in the lower areas near the river (graph opposite). Farr thought that cholera might be caused by breathing unclean air at lower altitudes. |
 |
During the 19th century, drinking water was supplied to houses by private companies via a network of pipes. There was competition between the water companies, resulting in overlap between the areas supplied by the different companies.
Toilets were widely introduced in London between 1830 and 1850: main sewers were introduced in the 1840s. The sewers emptied into the River Thames.
During the 1848-9 cholera epidemic, mortality from cholera was particularly high in the districts supplied by two particular water companies, the Southwark & Vauxhall and the Lambeth companies, both of which took water direct from the River Thames where it flowed through London.
Here is part of the original map of this area, including an area where both companies supplied water.

The green area was served by the Southwark and Vauxhall company, the pink area by the Lambeth company, and the grey area in between is where the two companies' pipes were intermingled.
Based on these observations, John Snow formulated a hypothesis on the nature and mode of communication of cholera:
- That cholera can be communicated from the sick to the healthy
- That disease is communicated by "morbid matter" which has the property of multiplying in the body of the person it attacks
- That the morbid matter producing cholera must be introduced into the alimentary canal
- Water supplies appeared to be able to disseminate the morbid matter from the sick to the healthy
There was no further cholera in London until 1853. During this period,
the Lambeth company moved its source so that it now drew water from the
Thames upstream of London (and thus uncontaminated by London sewage).
The Southwark and Vauxhall company continued to draw water from the Thames
in London. This provided John Snow with an ideal opportunity to test his
hypothesis.
![]() Now
work through the interactive exercise for this
topic
Now
work through the interactive exercise for this
topic
Exposures and Outcomes
The two key elements that we measure in most epidemiological studies are the exposure and the outcome.
|
The exposure is the risk factor that we are investigating, which may or may not be the cause |
|
|
The outcome is the disease, or event, or health-related state, that we are interested in |
An exposure can be any factor that may influence the outcome.
Take a moment to think of some exposures that may be relevant to whether or not a cow becomes infected with bovine tuberculosis, then compare them with our list below.
Exposures
|
Other infected cattle on farm |
|
|
Infected wildlife |
|
| Infection present in neighbouring herds | |
| Cow purchased from infected herd | |
| Cow tested false-negative |
These are just a few examples - you may have thought of others which are also correct.
The outcome can be any health-related event or state - or it can be a risk factor for, or a precursor to, a disease.
Examples
In a study of the effect of the presence of an infected wildlife species
in tuberculosis infection in cattle, presence of infected wildlife is
the exposure, or risk factor, that we are interested in, and the outcome
is tuberculosis infection in cattle.
However, in a study of the effect of soil type on tuberculosis infection levels in the wildlife species, the exposure of interest is soil type, and tuberculosis infection level in the wildlife is the outcome.
![]() Now
work through the interactive exercise for this
topic
Now
work through the interactive exercise for this
topic
Observational and Interventional Epidemiology
So far we have discussed one major type of epidemiological investigation: observational epidemiology, in which we describe patterns of health and disease of a population, without doing anything to change the factors which influence them.
Observational epidemiology includes both descriptive and analytical studies.
Observational epidemiology has its complications. In the real world, there may be more than one possible risk factor for an outcome. Inconveniently, these factors may be related to each other, and this can cause confusion.
Unless we take this problem into account, we cannot be sure that an association observed between an exposure and an outcome is genuine, and not the consequence of a third factor.
We will spend several sessions in this study unit (Chapters 9 to 12) discussing how to identify and avoid these and other potential pitfalls in epidemiological studies.
Example One
For example, William Farr found an association between elevation above
sea level and the risk of death from cholera. This association was because
it so happened that people living in the lower areas near the river were
more likely to be supplied with contaminated water.
So the apparent association between elevation above sea level and cholera was in fact caused by differences in water supply, which happened to be related to the elevation above sea level.
Example Two
As another example, if we did a study of the effect of milk production
levels on brucellosis infection in cows, we might find that there was
indeed an association where it appears that herds which produce more milk
per cow are more likely to become infected. But this could well be the
result of, for example, increased need for purchase of replacements in
order to improve the production potential of the herd.
So our finding of an association between milk production levels and brucellosis infection status of the herd may well be due to increased risk of purchasing infected animals, rather than due to the increased production levels themselves.
![]() Now
work through the interactive exercise for this
topic
Now
work through the interactive exercise for this
topic
What is the Role of Veterinary Epidemiology?
Veterinary epidemiology has three major functions:
|
To describe patterns of health and disease within populations |
|
|
To interpret these differences |
|
| To apply our results to improve animal health and welfare as well as protect public health and to evaluate the effect of health- and welfare-related interventions |
The first of these functions is to describe differences in the distribution of health and disease within and between populations.
With descriptive epidemiology, we can measure the burden of illness within a population.
For example, we might use descriptive epidemiology to examine how the pre-weaning mortality has changed in a particular country over the last 10 years, or to describe differences in the prevalence of hip dysplasia between various dog breeds, or to compare the incidence of bovine tuberculosis in different countries.
The second function is to interpret the differences we have described.
With analytical epidemiology, we can investigate risk factors for a disease or an outcome. Here we ask the question "does the pattern of exposure to certain risk factors among individual animals with or without a specific disease help us to work out the cause of the disease?"
For example, look at the maps of the global prevalence of Bovine brucellosis infection and of the incidence of Bovine tuberculosis illustrated here. Notice the similarity in the distribution of the high risk areas, suggesting that the two diseases are associated.

Bovine brucellosis cumulative incidence, 1995-99
(red -> higher risk)
Bovine tuberculosis cumulative incidence, 1995-99
(red -> higher risk)
This sort of analysis uses aggregated data, meaning data derived from whole populations rather than individual animals.
We can do similar analyses using data taken from individual animals rather than whole populations. For example, we might look at the effect of different levels of feeding dry cat food on the risk of a cat developing feline urological syndrome.
However, we must be careful in how we interpret our findings: in analytical epidemiology, we measure associations between exposures and outcomes. If we demonstrate an association, that does not necessarily mean that the exposure caused the outcome.
Example
The risk of bovine tuberculosis varies considerably by geographical
region, even within a single country. The risk of bovine tuberculosis
is higher in England than in Scotland. This does not necessarily mean
that for cattle to be kept in England causes bovine tuberculosis: it is
more likely that cattle in England are exposed to other factors which
are direct causes of bovine tuberculosis.
Later in the course (Chapter 21) we will discuss how to judge whether
an association is likely to be causal.
In some cases we can suggest appropriate preventive measures action even if we do not know the precise biological cause of a disease.
Example 1
We can reduce the risk of calf diarrhoea by feeding colostrum, even if
we do not know exactly what it is in colostrum that prevents calf diarrhoea.
Example 2
We can reduce the risk of respiratory disease in growing pigs by improving
the ventilation system of the shed, even if we do not know exactly which
pathogen causes the disease.
![]() Now
work through the interactive exercise for this
topic
Now
work through the interactive exercise for this
topic
Types of Epidemiological Investigation
We can summarise the main types of epidemiological
investigation in this diagram.
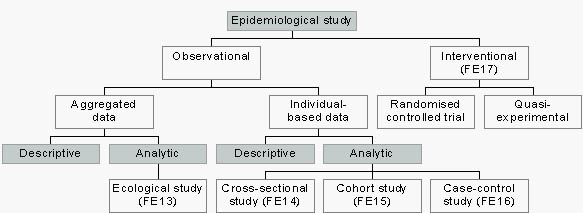
Observational study
A study in which the distribution of an exposure and/or an outcome
is examined without any attempt by the investigator to influence them.
Interventional study (Chapter 17)
A study designed to test a hypothesis by modifying an exposure within
the study population.
Aggregated data
Data concerning exposures and outcomes in which the unit of analysis is
the population rather than individual animals.
For example, we might examine data on the overall incidence of bovine spongiforme encephalopathy cases in different countries rather than in individual animals.
Individual-based data
Data concerning exposures and outcomes derived from individual animals
within the population.
Randomised controlled trial
A study in which individual animals are randomly assigned to receive the
exposure under investigation or to be a control who does not receive the
exposure. See Chapter 17.
For example, in a randomised controlled trial to investigate the effect of kennel cough vaccine in dogs coming to a boarding kennel, dogs were randomly assigned to receive the vaccine or to be a control (no vaccine).
Quasi experimental study
A study in which the investigator does not have full control over the
allocation of the exposure.
For example, a comparison of the incidence of bovine tuberculosis before and after the introduction of a control programme would be a quasi-experimental study.
Ecological study
A study in which data on average exposure and outcome for a population
are used to compare with similar data for other populations in order to
look for associations between the exposure and the outcome.
For example, in an ecological study of the effect of breed on risk of leg weakness in sows, the proportion of sows of a specific breed and the prevalence of leg weakness in different herds would be compared in order to look for an association. See Chapter 13.
Cross-sectional study
A study in which the prevalence of an exposure and/or an outcome are measured
in a given population at a specified point in time. The data may be analysed
to look for an association between the exposure and the outcome. See Chapter
14.
Example: the prevalence of Mycobacterium paratuberculosis infection in a particular herd could be determined by a descriptive cross-sectional survey. If data on possible risk factors for paratuberculosis infection are collected from the same animals at the same time then they could be used in an analytic study to look for associations between the risk factors and the disease.
Cohort study
A study in which one or more groups of individual animals are followed
up over a period of time to determine the frequency of a particular outcome
in the group(s).
For example, in a cohort study of the effect of the BSE disease status of the mother cow on the risk of BSE in her offspring, calves from diseased and non diseased cows were followed-up until disease occurrence. The frequency of BSE could then be compared between calves having a dam with or without BSE.
Case-control study
A study in which individuals with and without the outcome of interest
are identified. Their status with respect to exposures of interest is
then determined in order to look for associations between these exposures
and the outcome of interest.
For example, we could use a case-control study to determine risk factors for bovine tuberculosis in cattle at the herd level. We would identify herds with and without cattle tuberculosis and obtain information concerning exposures of interest (purchase, neighbours, wildlife). We would then analyse the data to see if presence of TB in neighbouring herds or frequent purchase of cattle was associated with bovine tuberculosis presence in the herd.
(No interaction for this topic at the moment)
Using Epidemiology to Investigate a Specific Disease Problem
Sometimes the investigation of a specific disease problem involves a sequence of epidemiological studies of different types. We can illustrate this with the example of the bovine tuberculosis in New Zealand.

Species involved in the epidemiology of bovine tuberculosis in New Zealand
Bovine tuberculosis has been controlled effectively in many countries around the world. Amongst the notable exceptions are several countries including the United Kingdom, Ireland and New Zealand, which have significant wildlife reservoirs of infection.
Wildlife reservoirs of infection can greatly influence progress of livestock disease control programmes, and they can also add a political challenge to the scientific problem which they already represent.
Disease problems which have single defined causes are relatively easy to eradicate, whereas true multi-factorial webs such as the case of bovine tuberculosis can appear to become insurmountable challenges.
In New Zealand, the Australian brushtailed possum is a major wildlife reservoir of bovine tuberculosis, but there are also other factors which contribute to continued presence of infection in the country, such as for example cattle movements, neighbourhood spread, false-negative tuberculin test results or other wildlife reservoirs.
The Sequence of Epidemiological Studies
1. Descriptive Studies
The prevalence of tuberculosis infection in New Zealand possums varies across the country. And it is often quite difficult to find infected animals, because the occur in small spatial clusters which it is easy to miss during a field survey.
One cross-sectional study conducted in the Central North Island of New Zealand determined a prevalence of 2.9% amongst 2900 possums examined.
2. Population-Based Analysis
The next step was to compare the association between prevalence of possum tuberculosis and cattle tuberculosis incidence between different regions around the country.
In other words, population-based analytic (ecological) studies were carried out, to examine the association between possum tuberculosis prevalence and the cattle tuberculosis incidence in several regions.
At this stage, populations were compared rather than individual animals, so this is an example of a population-based (or ecological study).
3. Individual-Based Analysis (Case-Control Studies)
As we will see later in the course, ecological studies have drawbacks and are better used to generate, rather than test, hypotheses. Further evidence is needed, in the form of individual-based analytic studies to confirm the suspected association.
Case-control studies were therefore carried out to establish the association between possum tuberculosis prevalence and cattle TB incidence at the individual farm level.
4. Intervention Studies
Once the association between possum and cattle tuberculosis was established, the next step was to apply this knowledge, and introduce an intervention. Experimental studies were carried out as part of the control programme, in the form of controlled trials, to investigate the effect of reduction of possum density on the incidence of cattle tuberculosis. Since it was important to obtain quick results, this phase was not planned as a formal investigation, but instead became a part of the disease control strategy. Currently, vaccination of possums is being evaluated using a series of experimental investigations.
5. Change in Disease Control Policy
Shortly after the link between possum and cattle tuberculosis was demonstrated, reduction of possum population densities became part of disease control policy.
6. Evaluation of the Disease Control Strategy
Once the benefits of population reduction have been established, the next stage is the evaluation of population reduction programmes.
This could be, for example, by monitoring the incidence of cattle tuberculosis in areas where population reduction has been implemented. Since such reductions will be implemented at specific points in time, temporal changes in cattle tuberculosis incidence in relation to recovery of the possum population can be monitored.
The Population Perspective
As epidemiologists, we deal with populations. Our basic questions with respect to an outcome in a population are "who, where and when"?
Epidemiology is sometimes criticised for having too narrow a focus, in that we identify and measure risk factors for a particular outcome, but tend to ignore the economic, historical, cultural or social context of those risk factors. Thus perhaps as well as "who, where and when?" we should be asking "and in what context?"
Epidemiological findings about risk factors such as type of pet food, pig barn ventilation system or dog breed are not always translated into effective disease prevention. This may be because we do not pay enough attention to the underlying economic or social processes that affect the distribution of these risk factors within a population.
These wider context of a disease problem may vary from one population to another, and this may need to be taken into account in developing strategies to control disease.
The medical epidemiologist Geoffrey Rose pointed out that we need to distinguish two types of determinants of disease in a population:
|
Factors that determine which animals within a population get a disease |
|
|
Factors that determine which populations get a disease |
For example, if we examine the association between badger
roadkill
tuberculosis prevalence
and bovine tuberculosis risk for cattle in Scotland, we will not detect
any effect, because there is no evidence of tuberculosis in badgers in
Scotland.
The effect can only be detected if we study a larger region with a wider range of exposure. Here is a graph of the correlation between badger roadkill tuberculosis prevalence and cattle tuberculosis incidence.

Relationship between badger roadkill TB prevalence
and cattle TB incidence in Great Britain
The graph shows a positive association between badger roadkill TB prevalence and cattle TB incidence - in other words, the more TB in badger roadkills, the higher the risk of cattle tuberculosis.
It follows that if we want to control disease on a population level, we need to understand the determinants of that disease at a population level, not just at an individual level.
For example, we might be asked to develop a disease
eradication strategy for bovine brucellosis. There are two approaches
that we could use:
|
|

In the previous example, a population strategy might be preferable since a high-risk strategy will not allow eradication of disease.
However, if the objective were to reduce infection prevalence in a cost-effective way, it may be more effective to target high-risk groups than to aim the intervention at the whole population. Modelling exercises may help to predict what strategy will be most effective.
Epidemiology is a young science that has developed particularly rapidly over the last 50 years, as new techniques of analysis have been developed. Much progress has been made, particularly in understanding the causes of infectious diseases (for example, the link between feeding of meat-and-bone-meal and BSE).
However new challenges continue to emerge. In recent years, for example salmonellosis campylobacter, scrapie and antimicrobial resistance have emerged as challenges to the animal and public health. As an epidemiologist, you are unlikely to become bored!
![]() Now
work through the Chapter exercises
Now
work through the Chapter exercises
Summary
This chapter has covered the following points:
What is veterinary epidemiology?
Veterinary epidemiology is the study of the distribution and determinants of animal health-, welfare- and production- related states or events in specified populations and the application of this study to control of health problems.
How do we describe an animal health-related event in a population?
The key elements are to describe the animal health-related event in terms of its distribution in time, place and animal.
Exposures and outcomes
An exposure is a risk factor for the outcome that we are investigating, which may or may not be the cause of the outcome.
The outcome is the disease, or event, or animal health-related state, that we are interested in.
Descriptive and analytical epidemiology
In descriptive epidemiology, we describe the distribution of an exposure or outcome, without seeking to explain the distribution by looking for associations.
In analytical epidemiology, we examine associations, often with the aim of identifying possible causes for an outcome.
Observational and interventional epidemiology
In observational epidemiology we examine the distribution or determinants of an outcome without any attempt to influence them.
In interventional epidemiology we test a hypothesis by modifying
an exposure within the study population and examining the effect on the
outcome.
Contents